로그인
로그인 회원가입
회원가입



Treatment Related Checklist
| Mesalazines |
|
||
|---|---|---|---|
| Steroid |
|
||
| AZA/6-MP* | Before initiating |
|
|
| While on therapy |
|
||
| Methotrexate | Before initiating |
|
|
| While on therapy |
|
||
| Anti-TNF (infliximab, adalimumab, golimumab) |
Before initiating |
|
|
| While on therapy |
|
|
|
| α4β7 integrin antagonist (Vedolizumab) | Before initiating |
|
|
| While on therapy |
|
||
| Anti-IL-12/IL-23 (ustekinumab), Anti-IL-23p19 |
Before initiating |
|
|
| While on therapy |
|
|
|
| JAK inhibitor (tofacitinib, upadacitinib, filgotinib) | Before initiating |
|
|
| While on therapy |
|
|
|
| S1P receptor modulator (ozanimod) | Before initiating |
|
|
| While on therapy |
|
|
|
| When IBD flare up |
|
||
*각 약제의 특성과 관련 없이 국내 결핵과 HBV, HCV발병률을 고려하여 Biologics 사용 전에 결핵과 HBV, HCV 항목 확인을 고려하며 관련 내용은 추후 변경될 수 있음.
Cancer Prevention
| Colon Cancer |
|
|---|---|
| Cervical Cancer |
|
Health Care Maintenance
| Education about vaccinations |
|
|---|---|
| Smoking cessation of CD patients |
|
| Nutritional Assessment |
|
| Depression/Anxiety |
|
Bone Health
| Vitamin D 25-OH level |
|
|---|---|
| Bone density Assessment |
|
| Prescription of Calcium & Vitamin D |
|
Appendix
*TPMT (thiopurine S-methyltransferase) and NUDT15 (Nudix hydrolase 15) testing before initiating AZA/6-MP
6-mercaptopurine을 6-methylmercaptopurine으로 분해하는 효소로, TPMT mutation에 의한 효소 활성도 감소는 thiopurine 연관 백혈구감소증을 흔히 유발한다.
서구에서는 TPMT mutation과 thiopurine연관 백혈구감소증과의 상관관계가 잘 정립되어, 미국 FDA 에서는 thiopurine 치료 시작 전 TPMT검사를 권장한다.
아시아에서는 서구에 비해 TPMT mutation 빈도는 낮은 반면 thiopurine 연관 백혈구감소증 발생률은 더 높다. 978명의 thiopurine 치료를 받은 한국인 크론병 환자를 대상으로 한 연구에서는 NUDT15유전자의 nonsynonymous SNP (p.Arg139Cys)가 thiopurine 연관 초기 백혈구감소증 발생과 강한 연관이 있음을 알아냄으로써 NUDT 15가 다양한 인구에서 thiopurine 연관 백혈구감소증 발생의 약물유전학적 결정인자임을 밝혔다 1,2.
아시아에서는 서구에 비해 TPMT mutation 빈도는 낮은 반면 thiopurine 연관 백혈구감소증 발생률은 더 높다. 978명의 thiopurine 치료를 받은 한국인 크론병 환자를 대상으로 한 연구에서는 NUDT15유전자의 nonsynonymous SNP (p.Arg139Cys)가 thiopurine 연관 초기 백혈구감소증 발생과 강한 연관이 있음을 알아냄으로써 NUDT 15가 다양한 인구에서 thiopurine 연관 백혈구감소증 발생의 약물유전학적 결정인자임을 밝혔다 1,2.
** Avoiding excessive use of steroid
스테로이드 불응(steroid-refractory)또는 의존(steroid-dependency)환자에서는 스테로이드를 tapering 하여 중지하고 immunomodulatory, biologics 등 steroid sparing treatment를 고려 이에 대한 기록을 남긴다.스테로이드 의존 (다음 항목 중 한 개 이상인 경우) 3
(1) 재발성 활동성 질환 없이 스테로이드 시작 후 3개월 이내에 스테로이드 용량을 프레드니솔론 10 mg/day 의 용량 미만으로 줄일 수 없는 경우; (2) 스테로이드 중단 후 3개월 이내에 증상이 재발하는 경우; (3) 1년 이내에 2회 이상의 스테로이드 사용하는 경우스테로이드 불응 3
: 4주 동안 프레드니솔론을 1 mg/kg/day까지 투여했음에도 불구하고 활동성 질환인 경우Steroid sparing treatment: 6-mercaptopurin 1.0-1.5 mg/kg daily: azathioprine 2.0-2.5 mg/kg daily: methotrexate 25 mg sc injection weekly: 또는 적정용량의 biologic therapy 4
*** Bone density assessment (BMD check): 다음에 해당하는 환자는 골밀도 평가를 해야 한다. 5
- 어떤 용량이건 스테로이드를 3달 이상 사용
- Inactive disease 상태이나 지난 2년 이내 최소 1년동안 장기적으로 스테로이드를 사용
- Inactive disease 상태이나 매우 마르거나 영양실조가 의심되는 경우
- Inactive disease 상태이나 무월경 상태인 여성
- 질환상태와 상관없이 폐경기 여성
† Extensive UC 및 colon involved CD 4
- 좌측 대장염(left-sided colitis) 또는 좌측 대장염보다 더 광범하게 침범된 궤양성대장염
- Colon의 1/3 또는 그 이상 광범위하게 침범된 크론병
†† 면역조절상태 6
-고위험 면역저하자
- Prednisolone 하루 20 mg에 상응하는 코르티코스테로이드제를 2주이상 투여 받는 중이거나 3개월 이내 중단한 경우
- 유효 용량의 면역조절제(MTX >0.4 mg/kg/week, AZA >3.0 mg/kg/day, 6-mercaptopurine >1.5 mg/kg/day) 또는 calcineurin 억제제(cyclosporines, tacrolimus) 투여 받는 중이거나 3개월 이내 중단한 경우
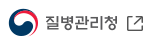
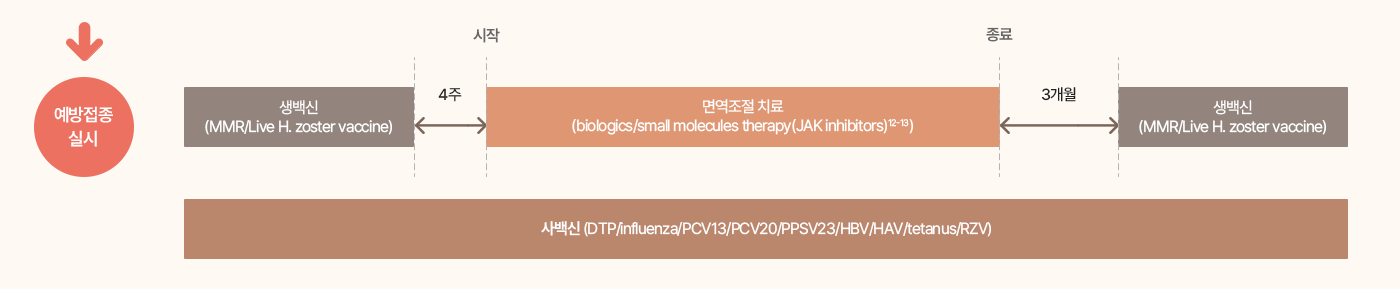
- 생물학 제제 또는 소분자 제제를 투여 받는 중이거나 3개월 이내 중단한 경우
- 저위험 면역저하자
- Prednisolone 하루 20 mg 미만에 상응하는 코르티코스테로이드제를 2주이상 투여 받는 중이거나 3개월 이내 중단한 경우
- 유효 용량의 면역조절제(MTX ≤ 0.4 mg/kg/week, AZA ≤ 3.0 mg/kg/day, 6-mercaptopurine ≤ 1.5 mg/kg/day)투여 받는 중이거나 3개월 이내 중단한 경우
- 기타 면역저하상태인 단백열량영양실조증, 비장기능저하증, HIV감염 등
* 본 checklist는 가이드라인과 새로운 약제의 추가 허가사항에 따라 변경될 수 있습니다.
Reference
- 대한장연구학회 IBD연구회, 크론병 치료 가이드라인. Korean J Gastroenterol 2012; 59(2):141-179.
- Yang SK et al. A common missense variant in NUDT15 confers susceptibility to thiopurine-induced leukopenia. Nature Genetics 2014;46(9):1017-1020
- Park Y et al. Physician education can minimize inappropriate steroid use in patients with inflammatory bowel disease: the ACTION study. Intest Res. 2022 Oct; 20(4): 452–463.
- Gil Y.Melmed and Corey A.Siegel, Quality Improvement in Inflammatory Bowel Disease. Gastroenterology & Hepatology. 2013 May; 9(5): 286-292.
- Cornerstones Checklist for IBD Patients. Version 1.4, updated9/4/2015. www.cornerstoneshealth.org
- Lee YJ et al. Vaccination strategies for Korean patients with inflammatory bowel disease. Korean J Intern Med 2022;37:920-930